What is prediabetes?
Prediabetes (also called non-diabetic hyperglycaemia) means your blood sugar is higher than it should be, but not high enough to be diagnosed as type 2 diabetes.3
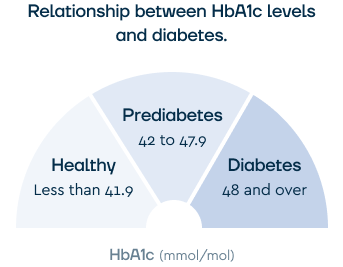
In the UK, it’s usually diagnosed using HbA1c, a blood test that reflects average blood sugar over the past 2 to 3 months. Diabetes UK and NICE use these ranges:3,4
- Normal: below 42 mmol/mol
- Prediabetes: 42 to 47 mmol/mol
- Type 2 diabetes: 48 mmol/mol or above
Some clinicians also use a fasting plasma glucose test.
A reading of 5.5 to 6.9 mmol/L is consistent with impaired fasting glucose, which sits in a similar risk band to an HbA1c of 42 to 47 mmol/mol.4
Prediabetes usually has no symptoms. Most people are picked up through routine NHS Health Checks, blood tests done for another reason, or screening if they have risk factors such as a higher BMI, a family history of type 2 diabetes, or South Asian, African, or African-Caribbean heritage.3
Risk of progression to type 2 diabetes
Without changes to lifestyle, weight, or medication, a meaningful proportion of people with prediabetes go on to develop type 2 diabetes.
Diabetes UK estimates that around 6.3 million UK adults are at increased risk based on raised blood sugar.2
Progression isn’t inevitable. The landmark Diabetes Prevention Program trial showed that intensive lifestyle changes reduced the incidence of type 2 diabetes by 58% over roughly three years compared with placebo.5
Is Mounjaro licensed for prediabetes?
No. Mounjaro is licensed in the UK for two indications:1
- Type 2 diabetes mellitus, alongside diet and exercise, in adults with insufficient blood sugar control
- Chronic weight management, alongside a reduced-calorie diet and increased physical activity, in adults with a BMI of 30 kg/m² or higher, or 27 kg/m² or higher with at least one weight-related condition
The Summary of Product Characteristics lists prediabetes as one of the weight-related conditions that qualify someone with a BMI of 27 or higher for the weight management licence.1
Prediabetes can therefore be the comorbidity that supports a weight management prescription, even though Mounjaro isn’t licensed for prediabetes alone.
Mounjaro on the NHS
NICE technology appraisal TA1026 sets out where tirzepatide can be funded by the NHS for weight management.6
Eligibility is more restrictive than the licensed indication and varies by area. Most people accessing it today do so privately.
NHS eligibility isn’t based solely on prediabetes. It depends on BMI, comorbidities, and local commissioning rules. Your GP or specialist team can advise on what’s available locally.
Mounjaro privately for prediabetes
Private providers can prescribe Mounjaro for weight management when you meet the BMI criteria. A reputable provider will:
- Confirm your BMI from measured height and weight
- Check your medical history, including eating disorders, gallbladder disease, pancreatitis, or thyroid concerns
- Review your prediabetes as the qualifying comorbidity if BMI is 27 to 29.9 kg/m²
- Provide structured support around food, activity, and behaviour change, not just the medication
If you’re taking other medications alongside Mounjaro, our GLP-1 medication compatibility checker covers the most common combinations.
How Mounjaro works
Mounjaro is a once-a-week injection that contains the drug tirzepatide. It mimics two gut hormones, GLP-1 and GIP, that communicate with the brain’s appetite centre to reduce hunger.
It also slows digestion, so food stays in the stomach longer. You feel full sooner and stay satisfied for longer after eating.
Tirzepatide also improves insulin action, which can bring blood sugar towards the normal range in prediabetes.
In the SURMOUNT-1 trial of adults with obesity, average weight loss at 72 weeks was 15.0% on 5 mg, 19.5% on 10 mg, and 20.9% on 15 mg, versus 3.1% on placebo.7
Evidence on tirzepatide and prediabetes
The clearest evidence comes from a long-term extension of SURMOUNT-1, which followed adults with obesity and prediabetes for 176 weeks (about three years).8
Over three years, 1.3% of participants on tirzepatide were diagnosed with type 2 diabetes, compared with 13.3% on placebo.
That’s a hazard ratio of 0.07, indicating a roughly 93% reduction in the risk of progression while on treatment.8
A meaningful number of participants also returned to normal blood sugar levels rather than just avoiding type 2 diabetes.
The published paper reports that the majority of participants treated with tirzepatide returned to normoglycaemia (healthy blood sugar levels), compared with a smaller proportion on placebo.8
After participants stopped tirzepatide and were followed for 17 weeks, the protective effect remained: 2.4% of those on tirzepatide developed type 2 diabetes, compared with 13.7% on placebo.8
Tirzepatide leads to substantial weight loss, and modest weight loss alone reduces the risk of progression to type 2 diabetes.5 Tirzepatide also improves the function of insulin, which helps the body manage blood sugar levels.
How this compares with lifestyle change alone
The Knowler et al. (2002) Diabetes Prevention Program trial showed a 58% reduction in the incidence of type 2 diabetes with intensive lifestyle changes over roughly three years.5
The NHS Healthier You programme has reported smaller real-world reductions, with completers around a third less likely to develop type 2 diabetes.9
Tirzepatide’s effect on diabetes incidence in SURMOUNT-1 is larger, but the trial population was specifically adults with obesity.
Lifestyle change is the foundation; the NHS DPP is the first-line offer; and medication can help when weight loss is a priority and someone meets the licensed BMI criteria.
Metformin and prediabetes
Metformin is the most commonly prescribed medication for type 2 diabetes in the UK.
It can also be used off-label in prediabetes, and NICE PH38 recommends it for adults whose blood glucose continues to deteriorate despite intensive lifestyle change, particularly those with a BMI above 35 or those at especially high risk of progression.4
The same Diabetes Prevention Program trial that established lifestyle change as a 58% effective intervention also tested metformin.
Metformin reduced the incidence of type 2 diabetes by 31%, a meaningful effect but smaller than that of the lifestyle arm.5
Metformin is inexpensive, widely available on the NHS, and well-tolerated by most people who take it.
It doesn’t support weight loss in the way tirzepatide does, though it can support modest weight loss in some people.
Discuss metformin with your GP if you have prediabetes and:
- Your HbA1c is rising despite lifestyle changes
- Your BMI is above 35
- You don’t meet the BMI criteria for tirzepatide
- You’d prefer an oral tablet to a weekly injection
The NHS Diabetes Prevention Programme
If your GP has told you that you have prediabetes, you may be eligible for Healthier You: the NHS Diabetes Prevention Programme.10
It’s a 9-month behavioural programme covering food, physical activity, and weight, delivered face-to-face or digitally.
Eligibility is usually based on a recent HbA1c of 42 to 47 mmol/mol or fasting plasma glucose of 5.5 to 6.9 mmol/L, with a GP referral. The programme has received over a million referrals to date.9
Second Nature is one of the lead digital providers of Healthier You and has worked with the NHS for over six years on diabetes prevention and weight management.
The NHS DPP and Mounjaro aren’t mutually exclusive. The DPP is a sensible starting point for most people, especially if BMI is below 30.
If you also meet the BMI criteria for weight management, talk to your GP or a specialist provider.
How often to retest your HbA1c
Once you have a prediabetes diagnosis, regular HbA1c testing tells you whether your changes are working.
NICE PH38 recommends at least an annual HbA1c for people identified as at high risk.4
In practice, most people benefit from earlier checks if they’re actively making changes:
- Lifestyle change alone, no medication: 6 months and 12 months after diagnosis, then annually
- NHS DPP completers: providers typically retest at the end of the programme (around 9 months) and at 12 months
- Starting Mounjaro for weight management: a baseline HbA1c, a check at 3 months, and then 6 to 12 monthly depending on your prescriber’s plan
- Starting metformin for prediabetes: typically a check 3 months in to confirm effect and tolerability, then annually
A reduction from the prediabetes range (42 to 47 mmol/mol) to below 42 mmol/mol is the goal of treatment. Your GP or specialist can interpret the trend, since a single test result can vary.
Foods to focus on with prediabetes
Diabetes UK’s eating advice for prediabetes focuses on whole foods, plenty of vegetables, fibre sources, and reducing ultra-processed and sugar-sweetened foods.3
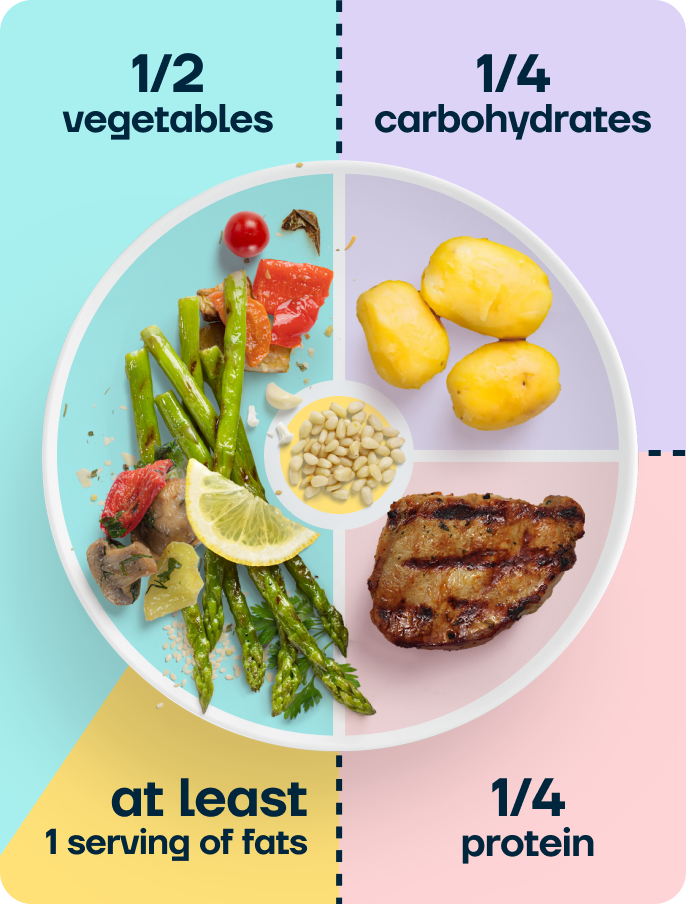
Second Nature’s approach uses the balanced plate model: half the plate vegetables, a quarter protein, a quarter complex carbohydrates, plus a serving of fat. It supports steady blood sugar without counting calories or following a strict diet.
Carbohydrate quality and post-meal blood sugar
Carbohydrates affect blood sugar more than any other food group.
Refined carbohydrates (white bread, sugary cereals, pastries, sugar-sweetened drinks) raise it quickly because fibre is removed in the refining process.
Complex carbohydrates with fibre (wholegrain or sourdough bread, rolled oats, brown rice, potato, sweet potato, quinoa, beans and lentils, wholemeal pasta) raise it more gradually.
The fibre is what slows the rate at which carbohydrates are digested. Fibre also feeds the bacteria in your gut, which produce short-chain fatty acids that improve insulin sensitivity over time (further improving blood sugar levels).
A practical approach for those living with prediabetes is to eat protein, fat, or fibre alongside any carbohydrate to help blunt the blood sugar rise.
A piece of toast with eggs raises blood sugar more gradually than toast with jam. Porridge with nuts and berries does the same compared with sugary cereal.
Sugar-sweetened drinks
Sugar-sweetened drinks (cola, lemonade, energy drinks, sweetened coffees) are the most direct way to raise blood sugar.
Swapping these for water, plain tea, or coffee is one of the highest-impact single changes you can make to manage blood sugar levels.
Eating 3 balanced meals, even when you’re not hungry
Mounjaro reduces appetite, which is part of how it supports weight loss. The challenge is to make sure the smaller amount you do eat still provides enough protein, fibre, vitamins, and minerals.
It’s essential to eat 3 balanced meals a day, even when you’re not hungry.
On days you’re when your appetite is very low, focus on smaller portions of nutrient-dense, whole food options like Greek yoghurt with berries, scrambled eggs on sourdough, or a spinach, banana, and protein powder smoothie.
Sleep and prediabetes
Short sleep duration (less than 6 hours a night) is associated with a higher risk of type 2 diabetes, independent of weight.11 Even a few nights of poor sleep can reduce insulin sensitivity in healthy adults.
Obstructive sleep apnoea, where breathing repeatedly pauses during sleep, is also strongly linked to insulin resistance and prediabetes.
It’s heavily underdiagnosed, particularly in people who don’t sleep with a partner who notices the breathing pauses.
If you snore heavily, wake unrefreshed, or feel sleepy during the day, it’s worth asking your GP about a sleep study.
Treating sleep apnoea improves insulin sensitivity, and weight loss reduces apnoea severity in most people.
Practical sleep targets:
- Aim for 7 to 9 hours a night, where possible
- Keep a consistent sleep and wake time, including at weekends
- Limit caffeine after early afternoon
- Reduce screens and bright light in the hour before bed
- Try relaxing activities in the hour before bed, like reading, yoga, or a hot bath
Movement and prediabetes
Physical activity directly affects blood sugar, regardless of weight loss.
When you move, your skeletal muscles absorb sugar (glucose) from the blood like a sponge, and keep doing so for hours afterwards. Regular movement also makes muscles more sensitive to insulin.
All movement helps our muscles burn sugar for fuel. Whether you’re going for a walk, shopping, or gardening, they all help to maintain healthier blood sugar levels.
Building a movement habit
Research by Lally et al. (2010) found that it takes an average of 66 days for a new behaviour to become automatic.12
Start with something so small it barely feels like effort, and attach it to something you already do.
A 10-minute walk after meals is a practical way to add more movement to your routine. As you start to feel more comfortable, you can make these walks longer.
Aerobic and resistance training
Aerobic activity (walking, cycling, swimming, dancing) lowers blood sugar during the activity and improves insulin sensitivity over time.
Resistance training (bodyweight exercises, resistance bands, or light weights) builds and preserves muscle.
Muscle is the main tissue that absorbs sugar from the blood, so more muscle means more capacity for clearing blood sugar after meals. It also helps preserve lean mass during weight loss on Mounjaro.
You don’t need a gym. Twice a week, a short session of squats, wall press-ups, glute bridges, and seated rows with a resistance band is enough.
Looking after your mental health
A prediabetes diagnosis can be unsettling. Some people feel motivated. Others feel anxious, judged, or overwhelmed by a ‘pre-disease’ label that hasn’t caused symptoms.
The psychological side of prediabetes doesn’t get talked about as much as the clinical side, but it affects how easy or hard it is to follow through on changes.
Motivation comes and goes
The early weeks after a diagnosis often feel motivating. Months in, when life gets busy, it’s normal for motivation to dip.
When motivation drops, what helps is having changes that don’t rely on you feeling motivated to do them.
Small actions tied to things you already do, like a morning walk, drinking water with meals, or choosing vegetables on half the plate, are easier to keep up than a strict plan.
Weight stigma and the prediabetes label
Many people with prediabetes also have a higher body weight. Weight stigma in healthcare and everyday life is well-documented and can make people avoid appointments, feel ashamed, or eat in response to stress.13
If you’ve felt dismissed by clinicians, it’s worth knowing that prediabetes is a chronic condition with multiple contributors, not a personal failing.
A clinician or programme that takes a non-judgemental, evidence-based approach gives you a better chance of sticking with the changes you decide to make.
When to speak to your GP
If you notice persistent low mood, loss of interest in things you used to enjoy, increased anxiety, disordered thoughts about food or weight, or thoughts of self-harm, speak to your GP.
You can also self-refer to NHS Talking Therapies for cognitive behavioural therapy and other talking therapies in most parts of England, without a GP referral.
Mounjaro vs Wegovy vs Saxenda
Mounjaro is one of three weight loss medications licensed in the UK. The table below compares them on the points most relevant to prediabetes.
| Medication |
Mounjaro (tirzepatide) |
Wegovy (semaglutide) |
Saxenda (liraglutide) |
| Mechanism |
Dual GLP-1 and GIP receptor agonist |
GLP-1 receptor agonist |
GLP-1 receptor agonist |
| Administration |
Injection, once a week |
Injection, once a week |
Injection, once a day |
| UK weight management licence |
BMI ≥30, or ≥27 with a weight-related condition (including prediabetes)1 |
BMI ≥30, or ≥27 with a weight-related condition |
BMI ≥30, or ≥27 with a weight-related condition. Branded Saxenda has been discontinued in the UK; generic liraglutide (e.g. Nevolat) is available |
| Average weight loss in trials |
15 to 20.9% over 72 weeks (5 to 15 mg)7 |
Around 15% over 68 weeks (2.4 mg) |
Around 8% over 56 weeks (3.0 mg) |
| Diabetes prevention evidence |
93% relative reduction in T2D incidence over 3 years in adults with obesity and prediabetes8 |
Reductions in HbA1c and progression risk reported in STEP trial extensions |
Reductions in diabetes incidence reported in the SCALE trial |
| Common side effects |
Nausea, diarrhoea, constipation, reduced appetite (typically most noticeable during dose increases) |
Nausea, diarrhoea, constipation, reduced appetite |
Nausea, diarrhoea, constipation, reduced appetite |
Tirzepatide currently has the largest reported diabetes prevention effect of the three.
None of these medications has been studied without support for diet and physical activity, so the trial results all reflect medication plus behaviour change.
Frequently asked questions
Is Mounjaro licensed for prediabetes?
Not for prediabetes alone. Mounjaro is licensed for type 2 diabetes and for weight management in adults with a BMI of 30 or higher, or 27 or higher with a weight-related condition.1
Prediabetes is a qualifying condition, so adults with both can be considered for the weight management licence.
How is prediabetes diagnosed in the UK?
Most commonly with an HbA1c blood test. A result of 42 to 47 mmol/mol indicates prediabetes (also called non-diabetic hyperglycaemia).3
Some clinicians also use fasting plasma glucose, with a prediabetes range of 5.5 to 6.9 mmol/L.4 Diagnosis is usually based on more than one test.
Can prediabetes be reversed without medication?
Yes, for many people. Intensive lifestyle change reduced the incidence of type 2 diabetes by 58% in the original Diabetes Prevention Program trial.5
The NHS Healthier You programme has shown smaller but meaningful real-world reductions.9 Losing 5 to 10% of body weight meaningfully lowers progression risk.
What about the NHS Diabetes Prevention Programme?
Healthier You is a 9-month NHS programme for adults with prediabetes, delivered face-to-face or digitally.10 Your GP can refer you.
It’s the standard first-line offer for most people in England with an HbA1c of 42-47 mmol/mol. Second Nature is one of the lead digital providers.
How much weight loss helps prediabetes?
Even modest weight loss helps. Losing 5 to 10% of starting body weight is enough to meaningfully reduce the risk of progression for most people.5
Mounjaro typically produces more weight loss, with an average of 15 to 20.9% over 72 weeks in trials.7
Can I get Mounjaro on the NHS for prediabetes?
Probably not on prediabetes alone. NHS access is governed by NICE TA1026 and local commissioning rules.6
Most people accessing Mounjaro today are doing so privately. Your GP can advise on local availability.
What about metformin?
Metformin is a low-cost oral medication that NICE PH38 recommends for prediabetes when blood glucose continues to deteriorate despite lifestyle change, particularly in adults with a BMI above 35.4
It reduced the incidence of type 2 diabetes by 31% in the original DPP trial.5
It doesn’t support the same amount of weight loss as tirzepatide, but not everyone needs medication, and it’s widely available on the NHS and a sensible option to discuss with your GP.
Will Mounjaro lower my HbA1c?
If you have prediabetes and lose meaningful weight on Mounjaro, your HbA1c is likely to come down.
In the SURMOUNT-1 long-term extension, 1.3% of people on tirzepatide developed type 2 diabetes over 3 years, compared with 13.3% on placebo.8
Can I stop Mounjaro once my HbA1c returns to normal?
This is a conversation to have with your prescriber. The SURMOUNT-1 extension found that some protective effect persists after stopping, with 2.4% of people who came off tirzepatide developing type 2 diabetes versus 13.7% on placebo at 17 weeks post-discontinuation.8
However, most people regain a proportion of weight when GLP-1 medications are stopped without sustained behaviour change.
A structured tapering plan and continued behaviour support give the best chance of holding onto the benefits.
Can I take Mounjaro if I’m planning a pregnancy?
Mounjaro isn’t recommended in pregnancy. If you’re planning to conceive, your prescriber will usually advise stopping it ahead of trying.
Prediabetes adds extra layers to consider, since higher pre-pregnancy HbA1c is associated with higher gestational diabetes risk.
Talk to your GP about preconception planning, and see our Mounjaro and pregnancy guide if it exists in the project.
Take home message
Mounjaro isn’t licensed for prediabetes alone, but it’s licensed for weight management in adults with a BMI of 30 or higher, or 27 or higher with a weight-related condition such as prediabetes.1
If you meet the BMI criteria, your prescriber can consider it under that indication.
For most people, weight loss and lifestyle change are the main approaches to lowering blood sugar levels.
Losing 5 to 10% of body weight, eating whole foods with plenty of fibre, prioritising sleep, and building a regular movement habit meaningfully lowers progression risk.5
The NHS DPP is the standard first-line offer in England, and metformin is a low-cost oral option NICE recommends when lifestyle change isn’t enough.4
Mounjaro can play a role when weight loss is the goal and the BMI criteria are met.
SURMOUNT-1 extension data shows a marked reduction in progression to type 2 diabetes over 3 years.8
Second Nature is one of the lead digital providers of the NHS Healthier You Diabetes Prevention Programme and runs a Mounjaro-supported weight management programme built around the balanced plate model (half vegetables, a quarter protein, a quarter complex carbohydrates, plus a serving of fat).
In a published service evaluation, active subscribers on Second Nature’s GLP-1-supported programme lost an average of 19.1% of their body weight at 12 months, with 77.7% achieving at least 10% weight loss.14
Second Nature's Mounjaro and Wegovy programmes
Second Nature provides Mounjaro or Wegovy as part of our Mounjaro and Wegovy weight-loss programmes.
Why choose Second Nature over other medication providers, assuming you're eligible?
Because peace of mind matters.
We've had the privilege of working with the NHS for over eight years, helping people across the UK take meaningful steps toward a healthier, happier life.
Our programmes are designed to meet people where they are, whether that means support with weight loss through compassionate one-to-one health coaching, or access to the latest weight-loss medications (like Mounjaro and Wegovy) delivered alongside expert care from a multidisciplinary team of doctors, psychologists, dietitians, and personal trainers.
At the heart of everything we do is a simple belief: real, lasting change comes from building better habits, not relying on quick fixes. We're here to support that change every step of the way.
With over a decade of experience, thousands of lives changed, and a long-standing record of delivering programmes used by the NHS, we believe we're the UK's most trusted weight-loss programme.
We hope to offer you something invaluable: peace of mind, and the support you need to take that first step.