What a trial average does and doesn’t tell you
An average is the total weight lost by everyone in a trial divided by the number of people. It’s a single figure for the whole group.
Averages are helpful because they show the medication’s overall effect. Across the group, people lost weight, which is the main evidence that the medication works.
But an average doesn’t tell you how much results varied from person to person.
In STEP 1, the main trial of Wegovy, average weight loss was 14.9% over 68 weeks.1 Some people lost much more, and some lost much less.
Proportions tell you more about what might happen to any one person. In STEP 1, 86% of people lost at least 5% of their body weight, 69% lost at least 10%, and half lost at least 15%.1
The placebo group shows how many people reached those thresholds without the medication.
| Weight loss |
On Wegovy |
On placebo |
| 5% or more |
86% |
32% |
| 10% or more |
69% |
12% |
| 15% or more |
51% |
5% |
Mounjaro produces a similar range of results, with more people losing larger amounts.
At the highest dose in SURMOUNT-1, 91% of people lost at least 5% of their body weight, and 57% lost at least 20%.2
| Weight loss |
On Mounjaro |
On placebo |
| 5% or more |
91% |
35% |
| 10% or more |
84% |
19% |
| 15% or more |
71% |
9% |
| 20% or more |
57% |
3% |
The Wegovy pill produces comparable results. In its main trial, the average loss was 13.6% across all enrolled participants, and 16.6% among those who remained on the pill and reached the full dose.3
These two figures represent different groups. The 13.6% includes everyone who enrolled, while the 16.6% includes only those who completed.
For how weight loss changes over time, use our free week-by-week GLP-1 timeline tool.
Why real-world results often fall short of the trials
Trial averages come from people who were supported to remain on the medication under research conditions and to reach the highest doses.
In the real world, it’s often more challenging to achieve the same level of weight loss we might see reported in a trial.
In a real-world study of nearly 8,000 people on semaglutide or tirzepatide, average weight loss at one year was 8.7%, well below the trial figures.9 This can be explained by a number of contributing factors:
- How well we tolerate the medication (impact of side effects)
- Whether we started developing healthy habits alongside the medication
- Whether we move up to the higher doses of the medication
- The difference in weight-loss goals (some people may wish to lose 5 kg, while others may target 20 kg)
- Baseline weight and other health conditions
In this real-world study, people who came off the medication within three months lost 3.6%, while those who stayed on it lost 11.9%. About 80% of patients stayed on the lower doses of the medication.9
So the trial averages describe something close to a best-case scenario in a very specific cohort of individuals living with obesity who are best placed to lose a lot of weight.
How much weight you lose ultimately depends on staying on the medication long enough to reach the dose that works for you and developing a healthier lifestyle alongside it to support overall health and reduce the risk of side effects.
Why averages describe groups, not individuals
The gap between what happens to a group and what happens to a person was explained well by the biologist Stephen Jay Gould.
In 1982, Gould was diagnosed with a rare cancer and read that the median survival was eight months. A median is the midpoint, with half of the patients above it and half below it.
Gould looked at the full range of outcomes rather than the midpoint alone. Half of patients lived longer than eight months, and some lived for years.
His age, early diagnosis and treatment placed him among the longer survivors, and he lived another twenty years.4
His essay on the experience, “The Median Isn’t the Message”, applies directly to weight-loss medication. As he put it, “variation is the hard reality” and “means and medians are the abstractions”.4
A trial average describes the group as a whole. It can’t predict how much any one person will lose, and individual results vary widely.
Plus, trial averages shouldn’t tell you how much to aim for. How much weight loss to target is a personal decision that should be based on a whole host of factors that go far beyond the average weight loss seen in research.
How much of the variation is down to the medication
Part of the difference between people isn’t associated with the effect of the medication at all.
In the same trials, about a third of people taking a placebo (a dummy version of the drug) lost at least 5% of their body weight, helped by being in a study, paying more attention to their habits, and the normal week-to-week fluctuation of weight.1
But the placebo effect is limited, as almost nobody taking a placebo lost 15% or more.
Small amounts of weight loss can be explained by many factors, but losses of 15% or more can, in most cases, be attributed to the medication.1,2
This variation of results has a recognised name in medicine: the heterogeneity of treatment effect. It means a single average can include people who respond strongly, people who respond only a little, and occasionally those who go the other way and respond badly to an intervention.
What determines an individual’s response
Part of the variation is biological. Genes influence how strongly the body responds to these medications, and researchers have begun to identify the specific genetic variants involved, which we cover in our piece on why GLP-1 medications work better for some people.
But our biology can only partly explain our weight-loss results, and it rarely predicts an individual’s result in advance. This is evidenced by a well-known diet study, DIETFITS, which tested whether biology could predict weight loss.
Stanford researchers set out to identify who would lose weight on a low-fat versus a low-carbohydrate diet from each person’s genetic profile and insulin response (a measure of how the body manages blood sugar).
Neither prediction worked. A person’s genes and insulin response didn’t predict how well they’d do on either diet.5
On the same diet, individual results over a year ranged from about 30 kg lost to 10 kg gained.5 The biology measured at the start couldn’t explain these differences.
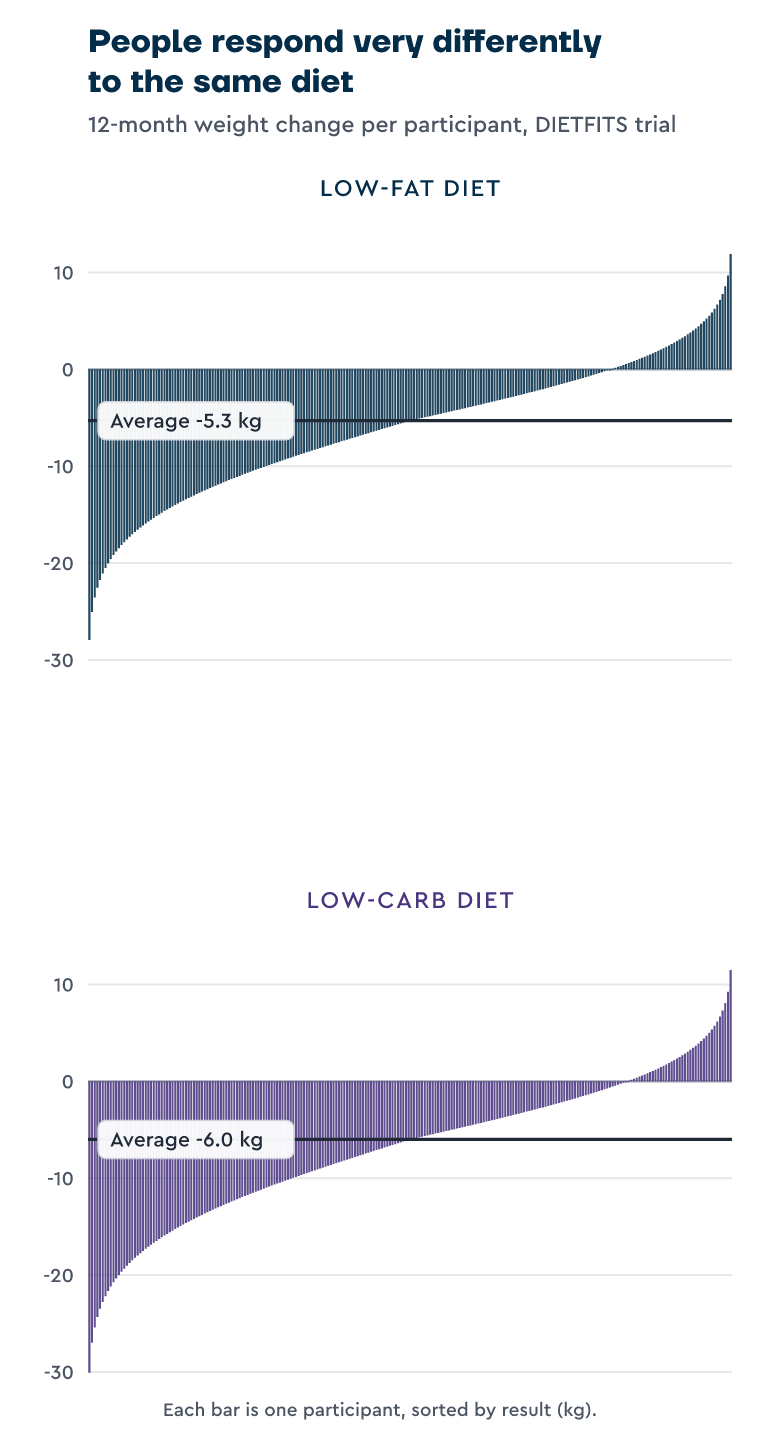
What had a greater influence on weight loss in either diet was behaviour. They ate more vegetables, reduced their intake of added sugars and refined grains, and cooked more whole-food meals at home.5
The same applies to GLP-1 medication. It reduces food noise, the constant thoughts about eating, which makes it easier to eat less.
While hunger and cravings are lower, it’s essential to develop a healthier lifestyle that will maintain weight loss in the long term if you decide to come off the medication.
It also depends on your relationship with food. Emotional eating, eating in response to stress or boredom, and meal routines all influence how much weight you lose and whether you can prevent weight regain.
Still, even if you choose to stay on the medication long term to manage hunger, your weight is only one of many factors that contribute to your health.
We’d still recommend eating a healthier diet, sleeping better, and developing psychological well-being to live a more meaningful and purposeful life.
If habits and diet quality are so important, why take the medication at all?
For many people, food noise is a persistent biological urge to eat that they’re helpless to ignore, rather than a lack of willpower, and it has undermined every previous attempt to eat differently.
The medication doesn’t change our behaviour. It quietens food noise, which, for many people, provides the first real opportunity to eat differently in their lives, because the constant pull towards food is finally reduced.
The time on the medication is the window to build those new habits and a better relationship with food, and those are what keep hunger and food noise lower if you come off the medication in the future.
Without those habits, stopping the medication suddenly typically results in weight regain.
In a follow-up to the STEP 1 trial, participants regained about two-thirds of the weight they had lost within a year of coming off semaglutide (Wegovy injections).11
This regain isn’t a failure of the medication, nor is it inevitable. But if we haven’t developed the healthier lifestyle to manage our hunger and cravings naturally, weight regain is more likely.
The people who maintain their weight loss are usually those who used their time on medication to change how they eat, move, sleep, and relate to food.
What improves weight-loss outcomes
Your response to GLP-1 medications usually becomes clear within the first few months. This is why UK clinical guidance in the NHS reviews progress at around six months and looks for at least 5% weight loss by that point.6
By then, you’ll usually have a good idea of how much you’re likely to lose. The things that improve your weight loss beyond this are mostly behavioural.
Getting enough protein helps protect your muscle while you lose weight, with a useful target of 1.2 to 1.6 grams per kilogram of body weight per day, or about a portion of protein the size of your palm at each meal.
Protein intake is crucial during weight loss, as it can help maintain muscle and other lean tissues, such as bone.
On these medications, most of the weight lost is fat, but some is muscle, which is why protein becomes so important.10
Additionally, it’s not just about muscle mass, but muscle function. Eating enough protein will help to protect mass, but it won’t improve the function and strength of our muscles. To achieve that, we need to be doing some form of resistance training.
Still, our diet isn’t all down to how much protein we eat. We recommend eating a balanced plate of roughly half vegetables, a quarter protein, and a quarter complex carbohydrates such as brown rice or potatoes, with a serving of healthy fat alongside.
This balanced approach to nutrition ensures we’re getting everything our bodies need to thrive, even as we naturally eat less as we lose weight.
Alongside diet and exercise, how we sleep and think also play crucial roles in our weight-loss success.
A comprehensive review published in Health Psychology Review analysed 26 studies on weight-loss maintenance.
The researchers identified many barriers to long-term weight maintenance, and most of these were psychological.
There were three main psychological barriers that people encounter when trying to maintain their weight loss:
- Old habits and impulses returning
- Having unmet needs
- Thoughts and beliefs about identity and weight
Our culture is obsessed with the notion that all we need to do is eat less and move more, and we’ll successfully lose weight and keep it off.
The truth is far more complicated. Of course, diet and exercise are important, but how we think, and our relationship with food and ourselves, are much more likely to predict whether we’ll successfully maintain weight in the long term than our understanding of what healthy food looks like.
The harsh reality is that most of us already know what a healthy diet looks like, but consistently applying it in our everyday lives over time is the challenge.
Additionally, if you stop the medication suddenly, without having developed a healthy lifestyle, some weight regain is likely, as our guide on coming off Mounjaro explains.
Still, a small number of people respond poorly to GLP-1 medications, whatever they do, also known as ‘non-responders’.
In the trials, about 1 in 7 on Wegovy and roughly 1 in 11 on Mounjaro didn’t reach the 5% weight loss considered a meaningful response.1,2
Losing almost nothing despite reaching the full dose is rarer, but it happens, and it’s the point at which your doctor may adjust the dose or consider a different approach to help you lose weight.
Making sense of your own weight loss
It’s easy to measure your own weight loss against the headline figures from the news, but those trial averages can be misleading.
If you purchase Mounjaro with a headline figure of ‘22.5% weight loss’, losing 8% may then feel disappointing, yet 8% is a meaningful outcome with clear clinical benefits.
Weight loss of over 5% is enough to lower blood pressure, improve blood sugar levels, and ease joint pain, and it falls comfortably within the normal range of responses.
Many people lose less than the average on the trial and still see significant improvements in their health.
We shouldn’t assume that a good outcome is defined solely by the total weight loss one has achieved.
Someone who has lost 6% of their body weight, and whose blood pressure has fallen, who now cooks from fresh ingredients on most days, and moves more regularly has built habits that will improve their overall health for the long term and reduce their risk of weight regain.
In comparison, someone who loses 18% without changing how they eat or move has not, and is more likely to experience weight regain and health complications in the future.
Comparing yourself to other people is just as misleading. Measuring your result against a friend’s, or against before-and-after photos online, compares just two results from a range so wide that one can’t predict the other.
The outcomes of others reflect their own body and circumstances, and a slower rate of loss is often more sustainable in the long run.
It also helps to follow the weight-loss trend rather than the daily number on the scales.
Weight naturally fluctuates by a kilo or two from one day to the next depending on what you’ve eaten, your salt intake, and hormonal changes, so a single weigh-in tells you very little. Judging your progress over time is far more reliable.
The most useful things to track are how your weight is trending over time and whether you’re experiencing other health benefits, such as moving more comfortably, lower blood pressure, your mood and optimism for the future, or clothes fitting more loosely. These are signs that you’re making progress and improving your overall health.
A genuine lack of progress is worth acting on, though. If you’ve been trying to lose weight for 6 months or more without seeing any progress, it’s worth raising it with your GP to discuss other options.
Our guides on not losing weight on Mounjaro and not losing weight on semaglutide cover the most common causes.
What weight loss is actually for
For most people, losing weight is a means to something else, whether that’s more energy, less joint pain, or independence and the freedom to live life in a way that’s meaningful to them.
That might mean climbing the stairs without stopping for breath, keeping up with your grandchildren, travelling comfortably again, or getting back to activities like hiking or skiing.
These improvements don’t depend on reaching a particular figure, and there are two distinct reasons why.
The medication itself does more than reduce weight. In a trial of 17,600 people with heart disease and obesity, semaglutide reduced the risk of heart attacks, strokes and cardiovascular death by about 20%, and that benefit was independent of weight loss.8
Those who lost less than 5% of their body weight saw the same cardiovascular benefit as those who lost more, suggesting a direct effect of the medication on the heart and blood vessels (possibly via the improvement in blood sugar and insulin levels) rather than a result of weight loss.
The habits we build alongside the medication improve our health in their own right. Eating more vegetables, cooking from fresh ingredients, moving more, and sleeping better lower blood pressure, ease joint pain, and improve blood sugar levels, whether or not they produce a large change on the scales.
In the STEP 1 trial, people’s physical functioning improved as they lost weight, and even modest weight loss eased joint pain and reduced the health risks associated with carrying extra weight.
Because the biggest health improvements don’t depend on reaching a particular percentage of weight loss, the average weight loss from a trial tells you even less about whether the medication is working for you than the headline figure suggests.
Weight loss is often talked about in terms of appearance. For most people, though, the changes that improve our quality of life are practical ones, like having more energy, more freedom, and getting back to the things we love doing but felt unable to do.
The number on the scale is only one part of the picture. What’s more important is what it gives back to you: your energy, your mobility, your independence. If those are improving, you’re succeeding, no matter how your results compare to a study average.
Frequently asked questions
Does Mounjaro work for everyone?
Almost everyone who takes Mounjaro loses some weight, but not the same amount.
In its largest trial, 91% of people on the highest dose lost at least 5% of their body weight, and more than half lost at least 20%.2 A small number lose very little, so while it works for most people, how well it works varies widely.
Why does Mounjaro work for some people and not others?
Part of it is biological, including genes that affect how strongly the body responds.
A large part comes down to what happens alongside the medication, such as how much you change your diet and whether you build lasting habits while taking the medication.
Why am I not losing weight as fast as other people?
Weight loss on these medications varies widely, even at the same dose, so losing weight more slowly than someone else usually reflects the normal range of responses rather than a sign that something’s wrong.
How long does it take to know if it’s working?
Most people get a clear sense within a few months. Response tends to appear early, and UK clinical guidance in the NHS reviews progress at around six months, looking for at least 5% weight loss by then.6
If nothing has changed by that point, it’s worth reviewing the medication with your prescriber or GP.
How do I know if I’m a non-responder to GLP-1 medication?
True non-response, losing almost nothing despite reaching a full dose over several months, is uncommon.
Most people who feel they aren’t responding are losing weight slowly rather than not at all, or are still early in the process.
Does it still work if I don’t change my diet?
Most people lose some weight regardless, because the medication reduces our hunger levels, no matter how we eat.
But the quality of our diet has a significant impact on our overall health, and while we may lose weight on the medication without changing our eating habits, we’re less likely to achieve our optimum health unless we also change our habits.
How much weight will I lose on the Wegovy pill?
On average, people lost 13.6% of their body weight in the Wegovy pill’s main trial, rising to 16.6% among those who stayed on it and reached the full dose.3
As with every medication we’ve discussed in this article, that average hides a wide range, with some people losing more than 20% and others less.
Can I do anything to make it work better?
Yes, if you develop a healthier lifestyle alongside the medication, you’re more likely to see better weight-loss outcomes and health improvements than if you simply use the medication but don’t change your lifestyle.
Take home message
The headline weight-loss percentages associated with weight-loss medications like Mounjaro, Wegovy, and the Wegovy pill don’t tell an individual what’s realistic for them or what their weight-loss goals should be.
Average weight loss from trials gives us an idea of how effective these medications are under controlled research conditions in a very specific cohort of individuals who are most likely to see significant weight loss.
Yet, they can’t tell us what a realistic weight loss is for an individual who’s going to take it in the real world.
Plus, the obsession with headline figures of ‘22.5% weight loss’ often clouds our understanding of what weight loss is actually for.
The purpose of weight loss is to improve our health, not to achieve the greatest possible weight-loss result.
Losing weight purely for the sake of losing weight is a bit like trying to drive as far as possible on a tank of fuel, rather than asking where you actually want to go. The distance only matters if it takes you somewhere meaningful.
At Second Nature, we pair medication with structured habit support to help people lose weight and improve their quality of life.
In a study published in JMIR Formative Research, active subscribers on the programme lost an average of 19.1% of their body weight at 12 months, with 77.7% reaching at least 10%.7
That 19.1% is an average too, drawn from active subscribers who stayed on the programme, so the same wide range of individual results applies.
Those results come from people using this kind of medication alongside habit support, which tends to reduce the risk of weight regain in the future.
Second Nature's Mounjaro and Wegovy programmes
Second Nature provides Mounjaro or Wegovy as part of our Mounjaro and Wegovy weight-loss programmes.
Why choose Second Nature over other medication providers, assuming you're eligible?
Because peace of mind matters.
We've had the privilege of working with the NHS for over eight years, helping people across the UK take meaningful steps toward a healthier, happier life.
Our programmes are designed to meet people where they are, whether that means support with weight loss through compassionate one-to-one health coaching, or access to the latest weight-loss medications (like Mounjaro and Wegovy) delivered alongside expert care from a multidisciplinary team of doctors, psychologists, dietitians, and personal trainers.
At the heart of everything we do is a simple belief: real, lasting change comes from building better habits, not relying on quick fixes. We're here to support that change every step of the way.
With over a decade of experience, thousands of lives changed, and a long-standing record of delivering programmes used by the NHS, we believe we're the UK's most trusted weight-loss programme.
We hope to offer you something invaluable: peace of mind, and the support you need to take that first step.























