What the evidence says
The most directly relevant evidence is a study by Hausner and colleagues, published in Clinical Pharmacokinetics in 2017.2
This study gave 26 healthy subjects a single 40 mg dose of atorvastatin, both with and without subcutaneous semaglutide at steady state.
The total amount of atorvastatin absorbed (AUC) was unchanged, with a ratio of 1.02, well within the 0.80-1.25 boundary that defines ‘no effect’. The time to peak blood level was delayed from 0.7 to 2.0 hours.2
Peak atorvastatin concentration (Cmax) decreased by 38%, but this was defined as not clinically relevant. Statin effectiveness depends on total exposure over time, not peak concentration.2
The same study also tested metformin, warfarin, and digoxin. All four drugs were within acceptable limits when taken with semaglutide.2
| Measurement |
With semaglutide |
Clinical significance |
| Total absorption (AUC) |
Ratio 1.02 (unchanged)2 |
No effect; well within acceptable limits |
| Peak concentration (Cmax) |
38% decrease2 |
Not clinically relevant; statin efficacy depends on total exposure, not peak levels |
| Time to peak (tmax) |
Delayed from 0.7h to 2.0h2 |
Reflects delayed gastric emptying; no impact on effectiveness |
While this study tested atorvastatin specifically, the same conclusion is expected for other statins (simvastatin, rosuvastatin, pravastatin).
Wegovy targets risk factors that statins don’t
Statins primarily lower LDL cholesterol, but they don’t address all cardiovascular risk factors.
Semaglutide improves several risk factors that statins don’t address. A meta-analysis of six randomised trials found that semaglutide 2.4 mg reduces systolic blood pressure by approximately 5 mmHg compared to placebo.8
The STEP 1 trial also showed reductions in CRP (a marker of inflammation) of 39-48%, alongside improvements in triglycerides, non-HDL cholesterol, and fasting insulin.4
| Risk factor |
Statins |
Wegovy (semaglutide) |
| LDL cholesterol |
Strong reduction (primary effect) |
Modest improvement through weight loss4 |
| Triglycerides |
Moderate reduction |
Significant reduction4 |
| Systemic inflammation (CRP) |
Moderate reduction |
39-48% reduction vs placebo4 |
| Blood pressure |
No direct effect |
~5 mmHg systolic reduction8 |
| Insulin resistance |
No direct effect (may slightly worsen) |
Improves blood sugar control and insulin function4 |
| Body weight |
No effect |
Significant reduction (9-15% typical)3,4 |
The two medications work on different aspects of cardiovascular risk. Statins lower LDL, while Wegovy improves weight, inflammation, triglycerides, and blood pressure.
The SELECT trial
The SELECT trial, published in the New England Journal of Medicine in 2023, is the strongest evidence that Wegovy and statins work well together.3
It tested semaglutide 2.4 mg in 17,605 people with established cardiovascular disease and a BMI of 27 or above, without diabetes. The average age was 61, and the average BMI was 33.3
Critically, 87% of participants were already taking statins. This means the cardiovascular benefits of semaglutide were measured on top of optimised statin therapy, not instead of it.
Key results
- 20% reduction in major adverse cardiovascular events (heart attack, stroke, or cardiovascular death)3
- 19% reduction in all-cause mortality3
- Average weight loss of approximately 9.4%3
For people already on statins who also have obesity, the SELECT data shows that adding Wegovy reduced their rate of heart attacks, strokes, and cardiovascular death by one-fifth, even though they were already receiving optimised statin therapy.3
Common side effects of both medications
Gastrointestinal symptoms
Nausea, vomiting, diarrhoea, and constipation are common with Wegovy. In the STEP 1 trial, nausea affected around 44% of people taking semaglutide 2.4 mg.4 Statins can also cause mild GI symptoms, but they’re far less common.
If you develop new GI symptoms after starting Wegovy, they’re almost certainly from the semaglutide rather than your statin.
Muscle symptoms
Muscle pain (myalgia) is the most talked-about statin side effect, but it’s less common than many people think.
An individual participant data meta-analysis of 23 large randomised trials (covering over 150,000 people) found that during the first year of statin therapy, the absolute excess of muscle pain or weakness was about 11 cases per 1,000 people per year. Only around 1 in 15 reports of muscle symptoms by people taking statins were genuinely caused by the statin itself.9
Semaglutide doesn’t cause muscle pain. If you develop new muscle symptoms, speak to your GP.
Fatigue
Both medications can contribute to tiredness. Fatigue from Wegovy is usually related to reduced calorie intake, particularly during the early weeks. Statin-related fatigue is uncommon. If tiredness persists, speak to your GP.
Foods to focus on
We recommend eating a diet based on whole foods that minimises the consumption of ultra-processed foods.
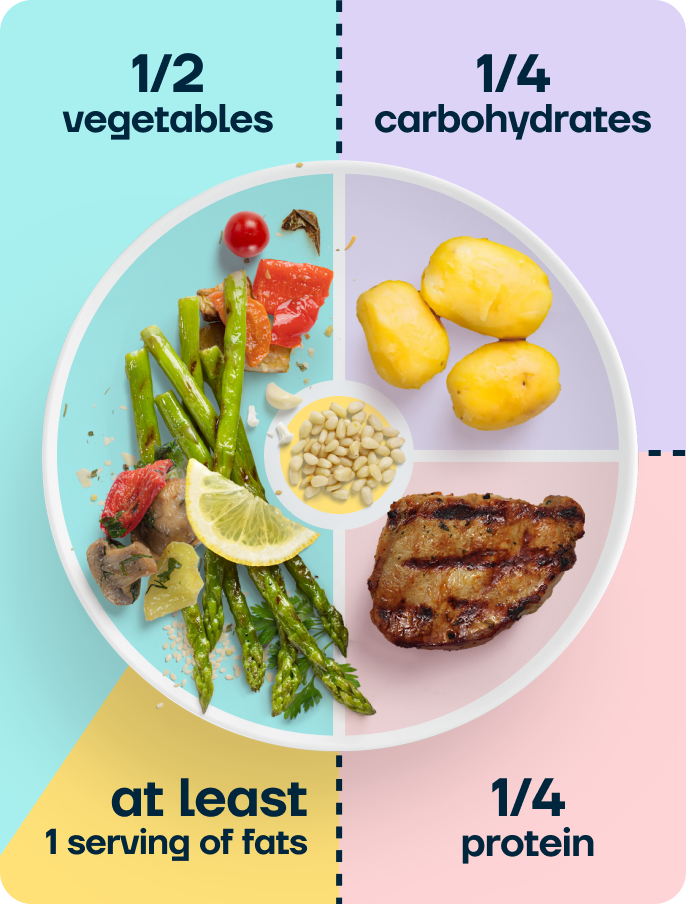
Our balanced plate model provides a framework for building balanced meals without counting calories or weighing food.
Aim for the majority of your meals to contain:
- 50% from non-starchy vegetables
- 25% from high-quality protein
- 25% from complex carbohydrates
- At least one serving of fat the size of your thumb (add more if your meals aren’t filling)
Heart-healthy protein and fats
- Oily fish (salmon, mackerel, sardines) at least twice a week for omega-3 fatty acids
- Lean protein at each meal: chicken, turkey, fish, eggs, red meat, lentils, tofu
- Extra virgin olive oil as a primary cooking fat
- Nuts and seeds (a small handful)
Complex carbohydrates and fibre
- Oats (a good source of beta-glucan, which reduces cholesterol absorption)
- Wholegrain or sourdough bread, brown rice, sweet potato
- Beans, lentils, and chickpeas for both fibre and plant-based protein
Vegetables
- Aim to consume a wide variety of vegetables over the week
- Colourful vegetables provide antioxidants that support cardiovascular health
Staying active
Regular movement is one of the most effective things you can do for cardiovascular health, alongside medication. It improves blood pressure and helps to lower blood sugar levels.
If you experience muscle symptoms on your statin
Some people worry that exercise will make statin-related muscle pain worse. Research suggests the opposite: a 12-week moderate-intensity exercise programme improved muscle strength and reduced fatigue in people experiencing statin-associated muscle symptoms, without worsening those symptoms.10
Staying active is important for the cardiovascular health that statins are prescribed to protect. If muscle pain is limiting your activity, speak to your GP. They may adjust your statin dose or try a different statin rather than have you stop exercising.
Getting started
The most important thing is building a habit you can sustain. Research on habit formation suggests that linking a new behaviour to an existing routine helps it become automatic over time.6 A 10-minute walk after dinner is a practical starting point.
Building strength
Resistance training helps maintain muscle mass during weight loss and has independent cardiovascular benefits.
Bodyweight squats, wall push-ups, or resistance band exercises are gentle starting points. You could try ‘exercise snacking’: a few squats while the kettle boils, or calf raises during a phone call.
When to speak to your GP
Contact your GP if you experience:
- New or worsening muscle pain, tenderness, or weakness (could indicate a statin-related issue that needs investigating)
- Persistent nausea or vomiting that prevents you from taking your statin consistently
- Dark-coloured urine alongside muscle pain (rare but warrants urgent assessment)
- Significant weight loss, as your statin dose or other cardiovascular medications may need reviewing
- Dizziness or lightheadedness, particularly if you also take blood pressure medication
- Feelings of anxiety or low mood related to managing multiple medications
Don’t stop taking your statin without speaking to your GP first, even if you’re losing weight and your cholesterol levels are improving. Your GP will review your cardiovascular risk and adjust medications as appropriate.
Frequently asked questions
Is it safe to take Wegovy with atorvastatin?
Yes. A formal medication interaction study found no clinically significant interaction between semaglutide and atorvastatin.
The total amount of atorvastatin absorbed was unchanged.2 The Wegovy SmPC confirms no dose adjustment is needed.1
Does it matter which statin I’m on?
The interaction study tested atorvastatin specifically, but the finding applies to all statins.2
Will Wegovy improve my cholesterol?
Semaglutide improves several lipid (blood fat) markers, including triglycerides and non-HDL cholesterol, through weight loss and direct effects like improved blood sugar levels.4
Some people taking semaglutide may be able to reduce their lipid-lowering medication over time, but this decision should be made by your GP.
Can I stop my statin if I lose weight on Wegovy?
Don’t stop your statin without medical advice. NICE guidelines recommend that statin therapy decisions should be based on a full cardiovascular risk assessment, not weight alone.5 While weight loss improves cardiovascular risk factors, statins provide independent benefits.
The SELECT trial showed that semaglutide’s cardiovascular protection was additive to statins, not a replacement for them.3
Should I take my statin at a different time from Wegovy?
There’s no need to change when you take your statin. Semaglutide’s effects on gastric emptying are continuous at steady state, not linked to the injection day. Continue taking your statin at your usual time.
Will I still get statin side effects on Wegovy?
Wegovy doesn’t worsen statin side effects. The two medications cause different types of side effects: Wegovy primarily causes GI symptoms, while statins can cause muscle symptoms.
If you develop new symptoms, your GP can help determine which medication is responsible.
Does the SELECT trial apply to me?
The SELECT trial studied people with established cardiovascular disease (prior heart attack, stroke, or peripheral arterial disease), BMI 27 or above, and without diabetes.3
If you match this profile and are already on a statin, the trial directly supports the benefit of adding Wegovy.
What about other cardiovascular medications?
Semaglutide has also been tested in combination with warfarin, digoxin, and metformin, with no clinically significant interactions.2
If you take blood pressure medication, your dose may need to be reduced as you lose weight. Your GP should review this.
Will Wegovy affect my CRP levels?
Yes. In the STEP 1 trial, semaglutide reduced CRP (a marker of systemic inflammation) by 39-48% compared to placebo.4
This anti-inflammatory effect complements the cardiovascular protection from statins.
Can I get Wegovy on the NHS?
Yes. NICE recommends semaglutide for weight management in eligible adults (TA875).
Your GP can refer you to a specialist weight management service. Taking a statin alongside Wegovy doesn’t affect your eligibility.
Take home message
Wegovy can be taken safely alongside statins, with a medication interaction study confirming no clinically significant interaction with atorvastatin.2
The combination is potentially complementary. Statins primarily lower LDL cholesterol, while Wegovy addresses weight, triglycerides, inflammation, and blood pressure, giving broader cardiovascular risk reduction.
The SELECT trial demonstrated that, in people with established cardiovascular disease, semaglutide 2.4 mg reduced major cardiovascular events by 20% on top of background statin therapy.3
Don’t stop your statin because you’re losing weight on Wegovy. The two medications work on different risk factors and provide additive protection.
Your GP should review your cardiovascular medications periodically as your weight changes.
Second Nature’s programme combines medication support with personalised nutrition guidance from registered dietitians and nutritionists, built around a balanced plate of vegetables, protein, complex carbohydrates, and healthy fats.
A peer-reviewed study published in JMIR Formative Research found that active subscribers on Second Nature’s semaglutide-supported programme lost an average of 19.1% of their body weight at 12 months, with 77.7% achieving at least 10% weight loss.7
Second Nature's Mounjaro and Wegovy programmes
Second Nature provides Mounjaro or Wegovy as part of our Mounjaro and Wegovy weight-loss programmes.
Why choose Second Nature over other medication providers, assuming you're eligible?
Because peace of mind matters.
We've had the privilege of working with the NHS for over eight years, helping people across the UK take meaningful steps toward a healthier, happier life.
Our programmes are designed to meet people where they are, whether that means support with weight loss through compassionate one-to-one health coaching, or access to the latest weight-loss medications (like Mounjaro and Wegovy) delivered alongside expert care from a multidisciplinary team of doctors, psychologists, dietitians, and personal trainers.
At the heart of everything we do is a simple belief: real, lasting change comes from building better habits, not relying on quick fixes. We're here to support that change every step of the way.
With over a decade of experience, thousands of lives changed, and a long-standing record of delivering programmes used by the NHS, we believe we're the UK's most trusted weight-loss programme.
We hope to offer you something invaluable: peace of mind, and the support you need to take that first step.