How the calculator works
The calculator estimates your daily calorie target in three steps.
First, it estimates your basal metabolic rate (BMR) using the Mifflin-St Jeor equation1. This is the number of calories your body burns at rest, just to keep you alive. It accounts for your sex, age, height, and weight.
Next, it multiplies your BMR by an activity factor based on your level of activity on a typical day.
The result is your total daily energy expenditure, or TDEE. This is the number of calories your body burns each day in total, including movement.
Finally, it applies a 10%, 12.5%, or 15% deficit to your TDEE to give you a daily calorie target. The default is 12.5%, which works out to around 0.5-0.7 kg of weight loss per week for most adults.
The calculator also estimates how the weight you lose will be split between fat and muscle over 12 weeks.
The default ratio is 75% fat, 25% muscle. This is the proportion observed in the SURMOUNT-1 tirzepatide trial across age, sex, and weight-loss subgroups, and was similar for placebo participants who lost weight without medication2.
If you eat enough protein and do some resistance training, you’re likely to lose more fat and less muscle.
For safety, the calculator won’t recommend a target below 1,200 kcal a day for women or 1,500 kcal a day for men.
If your TDEE is low and a 12.5% deficit would put your target below 1,200 kcal for women or 1,500 kcal for men, the calculator raises it back to that minimum.
Why we don’t recommend counting calories
While there can be some benefit to understanding how many calories you’re eating each day, we don’t recommend calorie counting.
The numbers themselves are imprecise
People consistently underestimate what they eat.
In a landmark 1992 study, obese adults with a history of failing to lose weight underreported their intake by an average of 47%3.
Underreporting in obese adults remains a consistent finding in more recent studies using doubly-labelled water (a way of measuring energy expenditure), although the average gap is smaller.
UK food labels are also legally allowed a 20% margin of error, and how much your body absorbs from a food varies. Adding imprecise numbers will give you an imprecise total.
How much you burn each day isn’t fixed
Sleep, stress, room temperature, how much you fidget, and the type of food you eat all change how much energy you burn each day. So a deficit that looks fixed on paper isn’t really fixed in practice.
It’s hard to keep up
Weighing every meal usually becomes a chore that many people give up on within a few weeks of starting.
Most people find it easier to lose weight when their approach doesn’t depend on tracking every meal.
Calories aren’t all equal
300 kcal of crisps and 300 kcal of eggs and avocado on toast affect your hormones, hunger, and metabolism differently.
What we eat has a significant impact on how our bodies respond, not just how much.
Counting can work well as a short stint to build awareness of portion sizes. But, for most of our members who come to us from a history of yo-yo dieting, the methods below are easier to keep up day-to-day.
If you’d like to learn more about why we don’t recommend calorie counting, see our guide on how to lose weight without counting calories.
How to reach your calorie target without counting
The balanced plate
We recommend that most of your meals should be made up of half your plate of vegetables, a quarter of complex carbohydrates, a quarter of protein, plus a serving of fat.
Using this approach, most meals fall within the right calorie range without needing to count or weigh anything.
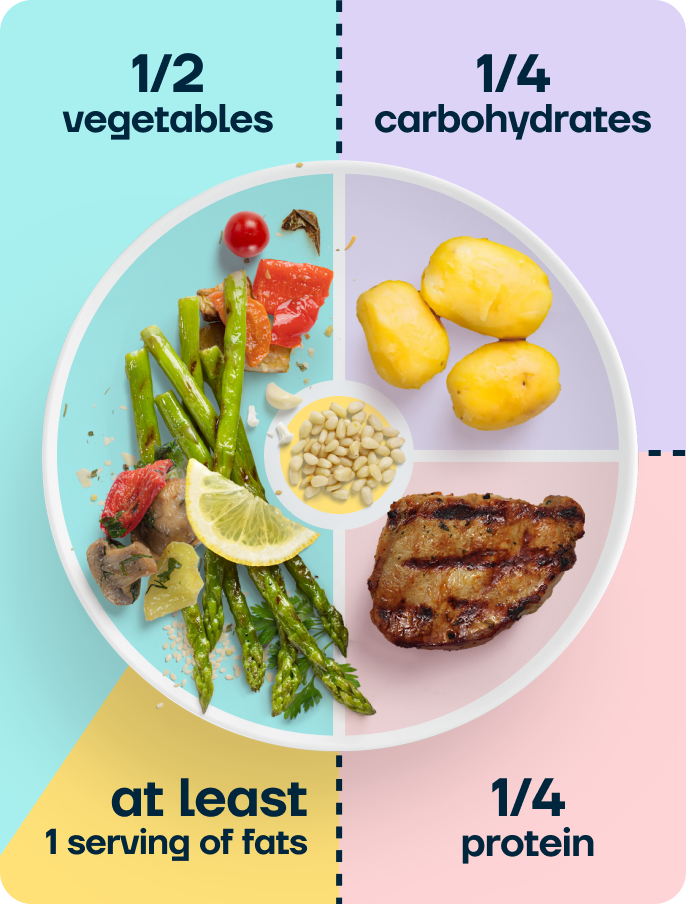
The balanced plate works because it controls for two things at once: the calorie density of what you eat (vegetables are low in energy, protein and carbohydrates are moderate, fats are high) and the balance of macronutrients (protein, fat, and fibre help you feel fuller for longer).
Members on our programme use this model at every meal, alongside the recipes in our app.
For an example of a balanced plate meal, see our Mexican pork bowl recipe: half the plate is salad, a quarter is brown rice, a quarter is chargrilled pork with black beans and tomatoes, plus the avocado as the fat serving.

Measure with your hands
Your hand scales with your body, so it gives you a fair guide to your own portion sizes. Per meal, aim for:
- One closed fist of complex carbohydrates (rolled oats, brown rice, sweet potato, wholemeal pasta, quinoa) 👊
- A palm of protein (chicken, fish, tofu, eggs, lentils) ✋
- Two open cupped hands of vegetables 🤲
- A thumb of fat (oil, nuts, butter, seeds) 👍
This works in all environments, whether you’re at home, in restaurants, or at someone else’s house.
Aim for around 30 g of fibre a day
The UK government recommends 30 g of fibre a day for adults, but the average UK intake is closer to 20 g10.
With GLP-1 medications, fibre intake often drops further as portion sizes shrink, which can worsen constipation (a common side effect of slowed gastric emptying).
Fibre also helps reduce hunger, so getting enough makes it easier to hit the calorie target.
Vegetables, wholegrains, beans, nuts and seeds, and pulses are the best sources of fibre.
Two cupped hands of vegetables at lunch and dinner, plus a portion of beans or wholegrains, will help most of us eat enough fibre each day.
Increase intake gradually if you’ve been eating less than 20 g a day, and drink enough water alongside.
If you increase your fibre intake too quickly, you may experience discomfort, such as bloating.
Make sure you eat enough, even if you’re not hungry
On a GLP-1, your medication reduces hunger and slows digestion, so you’ll usually get a clearer ‘I’m full’ signal than before.
Stop at the first signal of fullness rather than when the plate is empty. Eating past that point often leads to nausea or reflux later.
But if you’re losing weight too quickly, we’d recommend adding a protein-rich snack in between your main meals to ensure you’re eating enough to support sustainable weight loss.
The more common risk on a GLP-1 is undereating, especially of protein. The calculator gives you a daily protein target alongside the calorie target. Treat the protein figure as a daily minimum.
Research suggests that spreading protein across 3 to 4 meals slightly better preserves muscle than eating a large amount of protein in one or two servings9.
Around 30-40 g of high-quality protein per meal, 3 or 4 times a day, provides the body with enough protein from each meal to support muscle maintenance9. The calculator’s per-meal split supports this range.
If you’d like a deeper plan around protein and resistance training while losing fat, our free GLP-1 muscle and protein planner can help.
Why we cap deficits at 15%
We recommend a more sustainable weight-loss rate of around 0.5-1kg per week, as research suggests that losing weight faster than this can increase muscle and bone loss.
A 2011 study of elite athletes losing weight at different rates found that those losing weight slowly (around 0.7% of body weight a week) gained 2.1% lean mass over the study. Those losing twice as fast saw no increase in lean mass4.
A 2017 clinical trial in 36 obese and overweight adults reached a similar conclusion: slow weight loss preserved more fat-free mass and resting metabolic rate than rapid weight loss5.
Body composition data from the SURMOUNT-1 trial of tirzepatide show that approximately 75% of the weight lost was fat mass and 25% was lean mass2.
The same 75/25 split was observed regardless of age, sex, or the amount of weight participants lost.
It was also similar for people in the trial who lost weight on a placebo without the medication. This pattern of fat-to-lean loss appears to reflect general weight loss, rather than something specific to GLP-1 medications.
A 2024 review on how to limit muscle loss with GLP-1 medications found that eating enough protein and doing resistance training are the two most effective ways to protect muscle while losing weight6.
Additionally, a study on young men in a 40% calorie deficit who ate 2.4 g of protein per kg of body weight while doing resistance training gained 1.2 kg of lean mass over four weeks while losing 4.8 kg of fat7.
Without high-protein intake and resistance training, participants lost more muscle and less fat, as you’d expect.
Faster than around 1 kg a week means losing more muscle in exchange for a small additional amount of fat.
Keeping more muscle helps your body continue burning calories at a higher rate, making it easier to maintain your weight loss after you stop the medication.
After significant weight loss, your resting metabolic rate drops slightly more than body-size change alone would predict, an effect called metabolic adaptation8. Preserving lean mass blunts that drop, making it easier to maintain the lower weight.
For more on protecting muscle during weight loss, see our guide on how to lose fat, not muscle.
If you’re considering coming off your medication, our guide on coming off Mounjaro explains how to come off the medication without regaining weight.
Recalculating as you lose weight
The calorie target the calculator gives you changes as you lose weight. Your energy expenditure decreases because a smaller body burns fewer calories at rest and uses less energy to move around.
So a 12.5% deficit at your starting weight becomes a smaller deficit at a lower weight, even if your eating stays exactly the same. This is one of the reasons people often plateau around the 6 to 9 month mark on a GLP-1, especially as they approach the maintenance dose.
Recalculate every 5 to 10 kg of weight lost, or every 3 months, whichever comes first. Re-enter your current weight into the calculator and check whether the new target still suits your goals.
If your weight loss slows down, we don’t recommend eating less. It’s better to maintain a calorie deficit of around 10-15%, but allow time for your brain to reach its new set point.
Plateaus are a necessary part of a weight loss journey to allow your body to adjust to its new, lower weight. Over time, your body will start to burn excess fat again.
Calorie targets by medication
The calculator gives you a personalised target based on your details. For context on what people typically eat on each medication:
Mounjaro (tirzepatide)
Mounjaro typically reduces calorie intake by 30 to 40% in the first few months as the dose escalates.
Most people eat between 1,200 and 1,500 kcal per day at the maintenance dose, depending on their starting weight and activity level.
For more information on calorie intake, side effects, and what to do if you’re eating too little, see our guide on eating too little on Mounjaro.
Wegovy (semaglutide)
Wegovy reduces appetite slightly less than Mounjaro on average.
Most people on the 2.4 mg maintenance dose eat between 1,200 and 1,800 kcal a day. The new 7.2 mg dose, available since 2026, will lead to a similar reduction in energy as Mounjaro.
For more information on calorie intake while on Wegovy, see our guide on how many calories you should eat on Wegovy.
Ozempic (semaglutide for type 2 diabetes)
Ozempic contains the same drug as Wegovy (semaglutide) but is licensed for type 2 diabetes and has a lower maximum dose of 2 mg.
At equivalent doses, most people eat similar amounts to Wegovy users. For more details, see our guide on how many calories to eat on Ozempic.
Not on a GLP-1?
The calculator works for anyone losing weight, not just GLP-1 users.
The protein target drops to 1.2 to 1.6 g/kg (rather than the 1.6 to 1.8 g/kg recommended for GLP-1 users), and the guidance on using your medication for portion control doesn’t appear.
Everything else, including the calorie target and the balanced-plate methods, works the same way.
Factors that affect your calorie needs
Activity level
A sedentary 70 kg woman might need 1,800 kcal to maintain her weight; the same woman doing 5 strength sessions and 10,000 steps a day might need 2,300 kcal.
The calculator’s activity multiplier captures this, but if your activity changes day to day or week to week, your needs will shift too.
Body composition
Two people of the same weight, height, sex, and age can have different metabolic rates if their muscle-to-fat ratio differs.
Muscle uses more energy at rest than fat. The Mifflin-St Jeor equation doesn’t capture this directly, so people with more muscle than average tend to need slightly more calories than the calculator estimates.
Stage of GLP-1 treatment
GLP-1 medications lower hunger progressively as the dose increases. In the first few months, you might struggle to meet the calculator’s target because the medication makes you feel fuller faster.
At higher doses, you might find you’re able to eat more consistently as you adjust to the medication and how to balance intake with managing the drug’s side effects.
Sleep, stress, and life
Poor sleep increases hunger hormones (ghrelin) and reduces fullness hormones (GLP-1, CCK, PYY).
Chronic stress raises cortisol, which can increase cravings for calorie-dense food.
The calculator can’t include the impact of these factors, but both can meaningfully change how much you eat day to day.
Frequently asked questions
How many calories should I eat per day on Mounjaro?
The calculator gives you a personalised target based on your details.
For most adults, this works out to between 1,200 and 1,500 kcal per day at the maintenance dose, depending on starting weight and activity level.
For more on typical intake patterns, see our guide on eating too little on Mounjaro.
How many calories should I eat per day on Wegovy?
The calculator gives you a personalised target. Most people on the 2.4 mg dose eat 1,200 to 1,800 kcal a day.
See our guide on how many calories are in Wegovy for details.
Is a 1,200-calorie diet safe on a GLP-1?
For most adult women at moderate body weight, eating below 1,200 kcal a day for an extended period isn’t safe.
For men, the minimum intake would be around 1,500 kcal. Our calculator won’t recommend below those levels and will show a warning if your inputs would push the deficit lower.
What’s the maximum calorie deficit I should aim for on a GLP-1?
We cap our calculator at 15% below maintenance. Beyond that, the fat-loss benefit is small, but the amount of muscle you’d lose will increase4,5.
A 15% deficit translates to roughly 0.5 to 0.7 kg of weight loss a week for most adults.
Why does Second Nature cap the deficit at 15%?
Faster weight loss disproportionately comes from lean tissue, which protects your metabolism and helps you keep the weight off afterwards4,5,6.
Beyond a 15% deficit, you don’t lose much more fat, but you do lose noticeably more muscle and bone.
How much protein do I need on a GLP-1?
For most GLP-1 users, 1.6 g of protein per kg of body weight per day.
If you’re also doing resistance training, you might increase that to 1.8 g/kg.
The calculator gives you a daily total and a per-meal split (around 25-30 g of protein, 3-4 times a day).
If you want more detailed guidance on protein intake while taking GLP-1 medications, our muscle and protein planner provides it.
Why has my weight loss slowed down on Mounjaro or Wegovy after 6 months?
As you lose weight, your TDEE drops, so a deficit set at your starting weight gets smaller over time.
There’s also a small effect from metabolic adaptation, where your body burns slightly fewer calories than your new weight alone would predict8.
Recalculate using your current weight after losing 5 to 10 kg.
Do I need to count calories on Mounjaro or Wegovy?
No. The calculator gives you a target, but the methods on this page (balanced plate, hand portions, and tuning into your body’s hunger signals) are how most of our members reach it.
Counting works for some people in short stints to build awareness, but it isn’t the long-term approach we recommend.
How accurate is the calculator?
The Mifflin-St Jeor equation is the most accurate predictive equation for resting metabolic rate available, but it’s still an estimate.
It’s typically within 10% of measured values for most people1. Use the calculator’s number as a starting target, not a fixed rule.
Can I use the calculator if I’m not on a GLP-1?
Yes. Choose ‘Not on a GLP-1’ on the medication step. The protein target decreases accordingly, and the medication-specific guidance is hidden, but the calorie targets and balanced-plate methods work just the same.
Take home message
GLP-1 medications make it much easier to sustain a calorie deficit than a diet alone.
Beyond 15% below maintenance, though, the fat-loss benefit is small, and more of the weight you lose comes from muscle.
The calculator on this page gives you a personalised daily calorie and protein target, capped at 15% deficit, with a forecast of how the weight you lose will split between fat and muscle over 12 weeks.
At Second Nature, we don’t recommend counting calories because it’s imprecise, monotonous, and places too much focus on the numbers, which can take away our ability to tune into how different foods impact us.
Using our balanced plate model and hand guides to build meals is a much more sustainable way to lose weight in the long term.
Second Nature's Mounjaro and Wegovy programmes
Second Nature provides Mounjaro or Wegovy as part of our Mounjaro and Wegovy weight-loss programmes.
Why choose Second Nature over other medication providers, assuming you're eligible?
Because peace of mind matters.
We've had the privilege of working with the NHS for over eight years, helping people across the UK take meaningful steps toward a healthier, happier life.
Our programmes are designed to meet people where they are, whether that means support with weight loss through compassionate one-to-one health coaching, or access to the latest weight-loss medications (like Mounjaro and Wegovy) delivered alongside expert care from a multidisciplinary team of doctors, psychologists, dietitians, and personal trainers.
At the heart of everything we do is a simple belief: real, lasting change comes from building better habits, not relying on quick fixes. We're here to support that change every step of the way.
With over a decade of experience, thousands of lives changed, and a long-standing record of delivering programmes used by the NHS, we believe we're the UK's most trusted weight-loss programme.
We hope to offer you something invaluable: peace of mind, and the support you need to take that first step.























