What the study found
Researchers at the University of California, San Francisco, analysed MRI scans of the thighs of 615 adults participating in the Osteoarthritis Initiative, a US-based research programme.
None of the participants had signs of knee osteoarthritis at the time of their scans. On average, they were 60 years old with a BMI of 27.1
The team used T1-weighted MRI scans and a technique called Goutallier grading to measure the amount of fat visible inside the muscle tissue. They then compared these measurements to detailed dietary records covering the prior year.1
Ultra-processed foods made up around 41% of the average participant’s diet. It’s important to note that self-reported dietary records aren’t the most reliable way to understand eating patterns.
Still, we can at least be confident about the general proportions: on average, ultra-processed foods likely contributed a significant number of calories to the participants’ diets.
Higher ultra-processed food intake was associated with higher muscle fat storage across all thigh muscles measured (β = 0.108; P = .007), in the flexor muscles (β = 0.111; P = .008), and in the adductor muscles (β = 0.122; P = .004).1
In other words, people who ate more ultra-processed food had more fat inside their muscles even when their BMI, calorie intake, fat intake, activity levels, age, and background were taken into account.
The link was even stronger when the researchers used waist measurement instead of BMI as the body-size comparison, because waist measurement is a closer proxy for visceral fat (the fat stored in and around our organs).1
Beyond calories and nutrients
Most research linking ultra-processed foods to poor health has focused on calories and nutrients.
The standard explanation is that UPFs are energy-dense, low in fibre and protein, high in sugar and refined oils, and so they lead to overeating and weight gain.
The Radiology study is the first to identify additional fat storage within muscles, even when calorie intake is taken into account.
If UPF intake predicts muscle fat storage even when calories are matched, then something about ultra-processed foods appears to affect how the body stores and manages fat beyond their nutritional content alone.
Kevin Hall and colleagues at the US National Institutes of Health ran a tightly controlled four-week metabolic ward study in 2019, published in Cell Metabolism, which offered a suggestive parallel.
Twenty adults lived at the NIH Clinical Center and ate either an ultra-processed or a minimally processed diet for two weeks each.
The two diets were carefully matched for total calories offered, macronutrients, sugar, fibre, sodium, and energy density. Participants could eat as much or as little as they wanted.2
On the ultra-processed diet, participants ate approximately 500 kcal more per day, gained 0.9 kg over two weeks, and ate faster.
On the minimally processed diet, the same participants ate less and lost around the same amount of weight, without being restricted.2
This study was small (n=20), short (4 weeks), and conducted in a metabolic ward rather than a real-world setting.
Still, it was the first clinical trial to demonstrate that UPFs have a unique impact on how our body functions compared to whole foods.
| Study |
Design |
Finding independent of calories and nutrients |
| Hall et al. (2019), Cell Metabolism |
Metabolic ward RCT (n=20), 4 weeks |
Participants ate ~500 kcal/day more on a UPF diet matched for calories, macronutrients, sugar, fibre, sodium, and energy density2 |
| Akkaya et al. (2026), Radiology |
Cross-sectional MRI analysis (n=615) |
UPF consumption linked to greater intramuscular thigh fat, independent of BMI, calorie intake, fat intake, physical activity, and age1 |
Exactly why ultra-processed foods have this effect is still being researched.
Ultra-processed foods contain additives, emulsifiers, colourings, and flavourings not used in home cooking, and their industrial structure alters the food’s texture, palatability (enjoyment), and how it reaches the gut. Any of these factors might contribute to the effects observed in the two studies.
The ‘ultra-processed food’ category itself is debated among nutrition scientists. The NOVA classification, used by both the Radiology study and Hall’s work, groups foods by how they’re processed rather than by their nutritional content.
This means wholegrain bread and baked beans are grouped alongside crisps, biscuits, and fizzy drinks, even though intuitively, we might understand that there’s a difference between the potential of baked beans and crisps to impact our health.
The Lane et al. 2024 umbrella review itself pointed out that not all UPFs affect health in the same way.
Some sub-groups, including wholegrain bread, yoghurt, and dairy-based desserts, have actually been linked to better health outcomes when researchers break the category down.4
This is a real limitation of how we classify foods by level of processing.
At the same time, the same direction of effect is observed across dozens of studies, populations, and methods when examining overall UPF consumption, suggesting that the research is clearly pointing to harm from a higher intake, even if the classification is imperfect.
Intermuscular fat and health
The type of fat measured in the Radiology study is called intermuscular adipose tissue (IMAT).
It’s stored between and within muscle fibres, and it’s distinct from visceral fat (stored around the organs) or subcutaneous fat (stored under the skin).3
IMAT typically accounts for less than 5% of total thigh fat. Despite its small size, it’s strongly linked to insulin resistance, reduced muscle function, and poor health.
Higher IMAT is found in people with type 2 diabetes and metabolic syndrome, and it’s a predictor of surgical complications, poorer recovery from illness, and reduced mobility with age.3
Work led by Professor Bret Goodpaster has established IMAT as a distinct fat depot with its own biological properties.
It secretes inflammatory products called cytokines that can directly impair muscle insulin sensitivity, meaning muscles with more IMAT respond less well to insulin even when muscle mass appears normal.3
Two people with the same total muscle mass can have very different profiles depending on how much fat is stored within their muscle tissue.
The wider ultra-processed food evidence
A 2024 BMJ umbrella review combined 45 meta-analyses involving close to 10 million participants.
It found consistent associations between higher ultra-processed food intake and 32 adverse health outcomes, including cardiovascular disease mortality (about a 50% increased risk), anxiety and common mental disorders (48-53% increased risk), type 2 diabetes (12% increased risk), obesity, sleep problems, and depression.4
The Radiology study adds further evidence underlying the effect of UPFs on our health.
Taken together, the evidence shows that ultra-processed foods are associated with biological changes across multiple body systems, including cardiovascular, metabolic, mental, and musculoskeletal health.
The GRADE quality of evidence rating in the umbrella review was ‘low’ or ‘very low’ for most of these outcomes. This reflects the observational methodology available in this research area rather than the existence of the effect.
Individual effect sizes also vary widely. Some nutrition scientists have argued that the magnitude of risk for some outcomes (such as a 2% increase in all-cause mortality, or a 12% increase in type 2 diabetes) is small compared to established risk factors like physical inactivity.
The consistency of the direction of effect across dozens of independent studies is what gives the overall finding its weight, despite the limitations of individual studies.
What this means if you’re taking a GLP-1 medication
Maintaining muscle mass is already a priority for people taking GLP-1 medications such as Mounjaro (tirzepatide) or Wegovy (semaglutide).
Weight loss on these medications includes some loss of lean mass alongside fat mass, and protecting muscle requires adequate protein intake and regular resistance training.
The Radiology findings add a further consideration. If ultra-processed foods are independently associated with more fat inside muscle tissue, then how you eat during weight loss may affect not just how much muscle you keep, but the quality of that muscle and how well it functions.
In practical terms, this is further evidence that the quality of our diet is as important as the amount we eat.
Meals built around whole-food protein sources (eggs, fish, lean meat, Greek yoghurt, tofu, legumes), minimally processed carbohydrates, and vegetables may support muscle quality more effectively than a high-protein but UPF-heavy diet.
Limitations to keep in mind
The Radiology study was cross-sectional, meaning it captured a single point in time.
It can show an association between UPF intake and muscle fat storage, but it can’t prove that one caused the other.1
Reverse causation is a possibility. People who already have more intramuscular fat tend to be less physically active and less metabolically healthy.
The direction of effect could plausibly run the other way: underlying poor health leading to more UPF consumption, rather than UPFs causing the increase in fat storage in muscle.
Dietary intake was self-reported using food frequency questionnaires, which are known to be imprecise.
Dietary intake was self-reported using food frequency questionnaires, which are known to be imprecise. People who are more health-conscious tend to underreport how much UPF they eat.
Because the same people also tend to be more active and eat fewer calories overall, the statistical adjustments researchers make can’t fully separate one factor from another.
The ‘independent of calorie intake’ finding is only as reliable as the self-reported data behind it.
The participants were at risk for knee osteoarthritis, were on average 60 years old, and were predominantly American.
The findings may not generalise directly to younger adults, those without osteoarthritis risk, or to the UK population.
More research is needed to confirm causation, identify the specific mechanisms, and test whether reducing UPF intake leads to measurable changes in muscle fat storage over time.
What to do in practice
In the UK, ultra-processed foods account for approximately 54% of total calorie intake in adults.5
Because UPFs are in so many everyday foods, reducing them usually means changing what you buy, what you cook, and what you keep in the house.
Realistic starting points include:
- Swapping ultra-processed breakfast cereals for whole oats with fruit, Greek yoghurt, and nuts
- Cooking meals from single-ingredient foods rather than relying on ready meals
- Using whole yoghurt, nuts, fruit, and boiled eggs instead of packaged snacks
- Including a palm-sized protein source at each main meal (fish, meat, eggs, tofu, or legumes)
- Checking ingredient lists and being more cautious about products with long lists of additives, flavourings, and emulsifiers
The goal isn’t to eliminate UPFs completely. It’s to shift the overall pattern of the diet toward more whole foods.
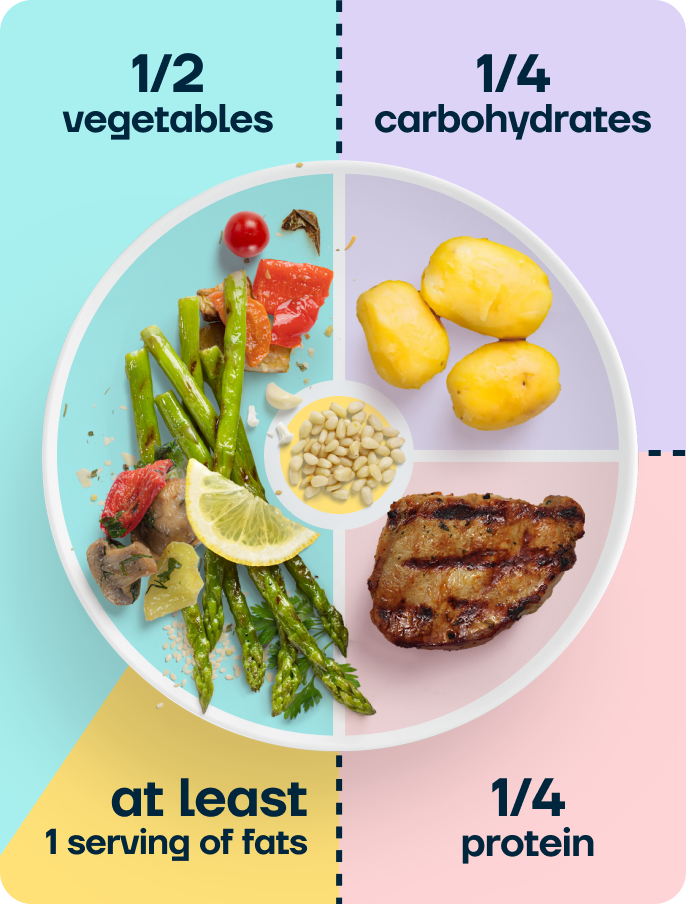
At Second Nature, we recommend our balanced plate model, which provides a foundation for most of our meals. We recommend most meals should contain:
- One fist of complex carbohydrates (25% of the plate)
- One palm-sized portion of protein (25% of the plate)
- Two open hands portion of vegetables (50% of the plate)
- At least one serving of fat the size of your thumb (one tablespoon of extra virgin olive oil)
Take home message
An MRI study of 615 adults, published in Radiology on 14 April 2026, found that higher ultra-processed food intake is linked to greater fat inside thigh muscle tissue, independent of calorie intake, physical activity, age, and BMI.
The type of fat measured, intermuscular adipose tissue (IMAT), is associated with insulin resistance, reduced muscle function, and poorer overall health.
The wider evidence that eating a lot of ultra-processed foods is linked to worse health outcomes is consistent across dozens of studies and multiple body systems.
The specific mechanism this study points to, muscle fat storage independent of calorie intake, is a newer finding and less firmly established.
The study is cross-sectional, the ‘ultra-processed food’ category itself has real limitations as a scientific classification, and the findings come from a specific older American cohort.
For anyone aiming to lose weight while preserving muscle quality, including people taking GLP-1 medications, the practical default remains what the broader evidence already supports: shift the overall diet balance towards minimally processed foods, without needing to eliminate UPFs completely.
Second Nature’s published research found that members taking semaglutide alongside dietitian-led behaviour change support achieved an average of 19.1% weight loss at 12 months.6